By Dr. Kaushik Vora, MS – Proctologist, Guwahati, Assam.
What is anal fistula?
Anal fistula is an abnormal tract connecting the inside of the anal canal to the skin around the anus. It causes symptoms like:
- Persistent discharge
- Pain and swelling
- Repeated abscesses
- Sometimes bleeding
Because it is a chronic disease, patients often look for a “permanent cure” and are easily attracted to words like “laser”, “scarless”, or “latest technology”.
Myth: “Laser fistula surgery has the highest success rate”
One of the most common beliefs today is:
“Laser is the best. If I do laser surgery for fistula, my success rate will be higher.”
This is not true.
Laser fistula surgery (commonly called FILAC – Fistula Tract Laser Closure) is heavily marketed as:
- Bloodless
- Painless
- High success
- Modern and superior
But in reality:
- FILAC has a high recurrence rate
- Many patients need repeat surgeries after laser procedures
- Laser is not the gold standard for fistula treatment
A lot of this is driven by marketing and propaganda from laser companies, not by strong scientific evidence.
What is the gold standard for fistula surgery?
According to multiple meta‑analyses and studies, the gold standard for fistula surgery is:
Fistulectomy – complete removal of the fistula tract.
Why?
- It removes the entire diseased tract
- It allows proper assessment of internal opening
- It reduces the chance of hidden residual tract
However, there is an important catch.
Then why do fistulas still recur after fistulectomy?
You might wonder:
“If fistulectomy is the gold standard, why do so many patients still have recurrence?”
The answer lies in how the fistulectomy is done.
Complete vs incomplete fistulectomy
- Complete fistulectomy → entire tract removed → higher success rate
- Incomplete fistulectomy → part of the tract left behind → recurrence
In many cases, especially in complex fistulas, a portion of the tract remains inside the sphincter muscle and is not removed completely.
Understanding trans‑sphincteric fistula
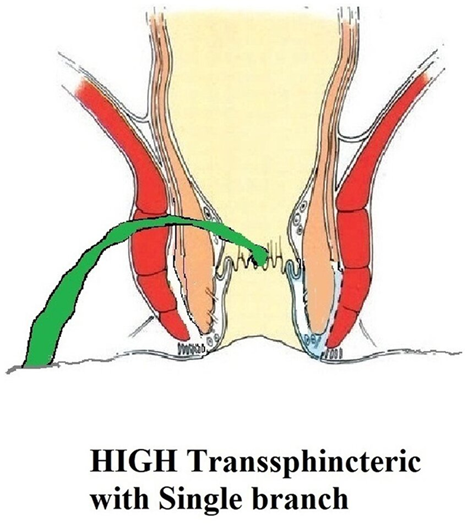
A trans‑sphincteric fistula means:
- The fistula tract travels through the sphincter muscle (the muscle that controls continence).
In such cases, during fistulectomy:
- The sphincter muscle has to be cut to remove the entire tract
- After cutting, the sphincter must be properly repaired
This requires specialised training in:
- Sphincter repair techniques
- Anorectal reconstruction
Why recurrence happens in trans‑sphincteric fistula
If the surgeon:
- Is not confident in sphincter repair
- Fears cutting the sphincter (to avoid incontinence)
- Leaves the intra‑sphincteric portion of the tract behind
Then:
- A part of the fistula tract remains
- This residual tract continues to cause infection
- The fistula recurs, even after “fistulectomy”
So the problem is not the name of the surgery, but whether the entire tract is removed and repaired correctly.
Laser vs fistulectomy: what patients should really know
Laser (FILAC):
- Uses a laser fibre to burn the tract from inside
- Often does not remove the entire tract
- Has higher recurrence rates in many studies
- Is attractive because of the word “laser”, but not necessarily superior
Fistulectomy (complete):
- Removes the entire fistula tract
- When done properly, offers higher long‑term success
- Requires skill in sphincter handling and repair, especially in trans‑sphincteric fistulas
Key takeaways for patients
- Laser is not a magic wand for fistula.
- FILAC has high recurrence and is not the gold standard.
- Fistulectomy is the gold standard as per meta‑analyses, but only when done completely.
- In trans‑sphincteric fistula, proper sphincter cutting and repair is crucial.
- Recurrence often happens when the intra‑sphincteric portion of the tract is left behind.
When you choose fistula surgery, don’t just ask:
“Is it laser?”
Ask:
“Will the entire tract be removed?” “Is the surgeon trained in sphincter repair?” “What is the long‑term success rate of this technique?”
That’s where the real difference lies.